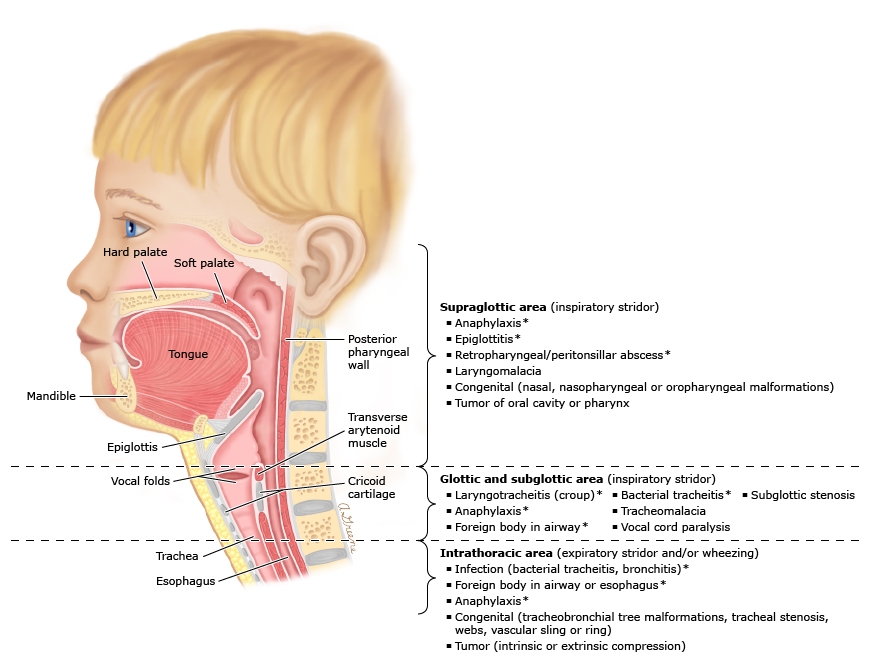
Acute Stridor is a harsh, grating respiratory noise that can often be heard without a stethoscope and is caused by airflow obstruction through the upper airway. The noise is caused by rapid and turbulent flow through a narrowed airway. The most common causes of stridor in infants without fever include congenital malformation of the airway or compression of the airway by other great structures around the airway, subglottic stenosis, laryngomalacia, tracheomalacia. In older children viral or bacterial infection in the airway, foreign bodies or other anatomic issues such as laryngeal cleft or bronchogenic cyst can cause this noise. The cause of this noise varies by age but the predominant clinical symptom is the same. We will be discussing acute stridor in children in this article, stridor in infants will follow in the series.
The noise is caused by rapid and turbulent flow through a narrowed airway.
Listen: Audio of Acute Stridor in Children
Causes of Acute Stridor Based on Anatomy
Acute Stridor
Acute Stridor, the topic of this article, is often of quick and dramatic onset making anatomic issues less likely and infectious causes and foreign bodies more common.
Laryngotracheitis
Laryngotracheitis / Viral Croup
Laryngotracheitis or Viral Croup develops over hours to days in children with previous upper airway infection. It typically affects children 6 months to three years old. Runny nose, fever and stridor are all usually present. It is a self-limited disease that ususaly resolves in 3 to 5 days.
Bacterial tracheitis
Bacterial Tracheitis
Bacterial tracheitis is generally, happens in the first 6 years of life. Most children have a URI prodrome but then present with severe respiratory distress, anxiety secondary to shortness of breath and fever. They may also have drooling, muffled voice and their position of comfort is upright. Much like classic H. flu epiglottitis of the past prior to vaccine availability. It is treated with controlled airway management and IV antibiotics in the Pediatric Intensive Care Unit. The airway is assessed intermittently by ENT to assess readiness for extubation.
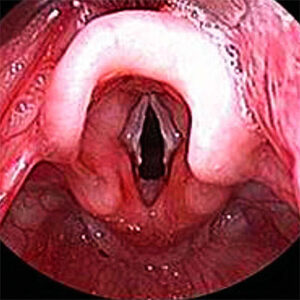
Epiglottitis
Epiglottitis
Epiglottitis is an inflammation or infection of the epiglottis which is the structure that protects the trachea during swallowing. Inflammation of this structure can cause acute airway obstruction and be deadly. Children present with anxiety, severe respiratory distress, drooling and muffled speech. Classically this has been caused by H. Influenza however since the development of a vaccine incidence of epiglottitis has dropped dramatically. It can be caused by virus as well but this is much less common. Treatment of viral epiglottitis is airway management and supportive care. In the case of classic epiglottitis IV antibiotics are added to the care plan.
Retropharyngeal abscess
Retropharyngeal Abcess
Retropharyngeal abscess occur between ages 2 years to 5 years old. May be indistinguishable from peritonsillar abscess or uncomplicated pharyngitis but as the disease progresses fever and drooling become more evident and inspiratory stridor. CT with IV contrast will help make the diagnosis. Treatment is IV antibiotics and surgical drainage.
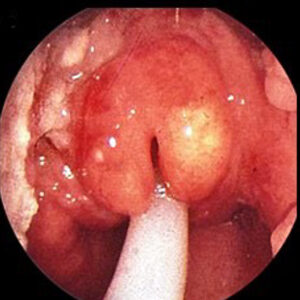
Peritonsillar abscess
Peritonsillar Abcess
Peritonsillar abscess arising as a complication of pharyngitis or tonsillitis, usually peaks in children about 10 years old when streptococcal pharyngitis peaks. Typically presents with severe sore throat (usually one side worse than other), fever, muffled voice, drooling, neck swelling. Treatment is IV antibiotics and surgical drainage.
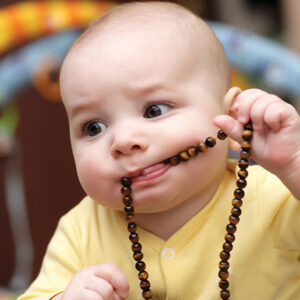
Foreign Body Aspiration
Foreign Body Aspiration
Foreign body aspiration should always be suspected in infant or toddler with acute airway compromise but this often does not present with fever. Incidence peaks about 3 years old Witnessed choking helps make the diagnosis but this is often not the case and not all FB are radio-opaque (able to be seen on x-ray) so high index of suspicion is necessary.
Anaphylaxis
Anaphylaxis
Anaphylaxis is commonly caused by food or medications. It is a severe and life-threatening swelling of the airway that involves the retropharynx (back of the throat) and the larynx (the voice box). It commonly has severe acute respiratory symptoms after ingesting the offending trigger substance but the child may also have hives, itching and mouth swelling as well as diarrhea, vomiting and abdominal pain. Treatment includes IM epinephrine immediately to slow airway swelling, glucocorticoids, H1 /H2 antihistamines help with itch but do not relieve airway swelling, sometimes bronchodilators may be used as well. Airway protection may be necessary.