
By Santa J. Bartholomew M.D. FAAP, FCCM
Toddlers and young children often put things in their mouth and are also unable to tell care providers, both family and healthcare, what they put in their mouth, so it can be a challenge to decide what needs to be removed quickly and what can move through the gastrointestinal tract. Unfortunately, even benign foreign bodies that may not cause harm to the child often get caught at the proximal esophagus or mid-esophagus (near the aortic arch) and cannot pass into the stomach.
Even benign foreign bodies that may not cause harm to the child often get caught at the proximal esophagus or mid-esophagus and cannot pass into the stomach.
The Most Common Foreign Bodies + Care
COINS — The most commonly ingested objects in children in the United States. In about 30% of children these pass spontaneously- once the coin passes to the stomach it is very likely to clear without issue. Since Canadian quarters are larger than US coins, they more often need to be removed endoscopically particularly in children under 5 years old.
- Children may be asymptomatic or may present with drooling, pain on swallowing or respiratory distress.
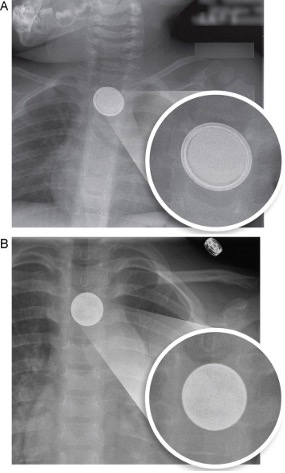
- Evaluation should include chest, abdomen x-rays both AP and lateral to determine coin from batteries.
- Treatment: Coins lodged in the esophagus should be removed within 24 hours to minimize the risk of esophageal erosion or injury. Coins that have already entered the stomach can be observed without intervention unless there is unremitting abdominal pain.
BUTTON BATTERIES — The most common batteries found in a household are found in watches, toothbrushes, toys, and musical greeting cards. The ingestion of a button battery is a medical emergency.
Once the battery contacts the esophageal mucosa it makes hydrogen radicals which result in chemical damage to the esophagus. Second, the electrical current that occurs when both sides of the batteries touch the wall of the esophagus can also damage the esophagus. In animal models, these injuries can occur within 15 minutes of ingestion.
- The change in batteries for toys and watches from 3V to 20mm lithium button batteries has led to a significant increase in ingestions.
- Children typically present with drooling, fussiness, fever, refusal to feed, and respiratory distress/stridor.
- Plain X-rays should be obtained in all suspected ingestions- clues on x-ray to a button battery may be a halo sign or double shadow.
- Esophageal battery ingestions should be removed within 2 hours regardless of the presence of symptoms or not.
- If the battery has left the esophagus it can be observed for 72 hours and the use of Carafate or honey to neutralize the pH is now recommended.
- Button battery ingestions have many morbidities even when handled appropriately from both the pH and the electric charge such as tracheoesophageal necrosis and subsequent stricture, vocal cord injury, aorto-enteric fistula, and mediastinitis.
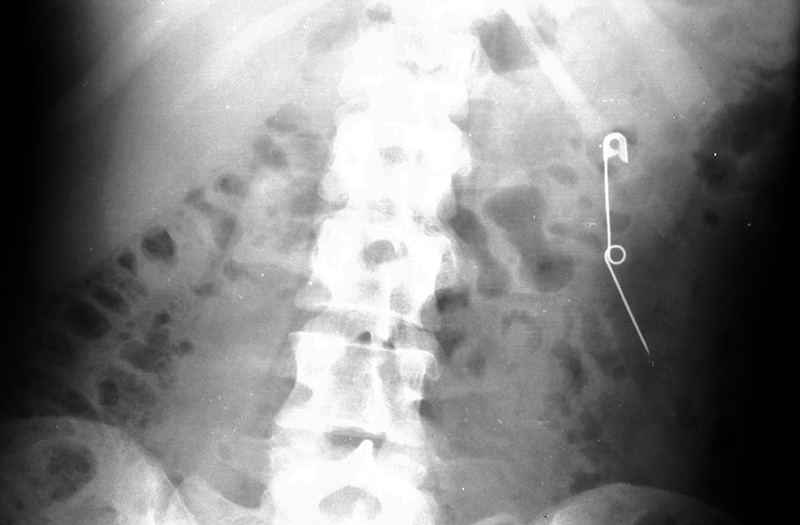
SHARP OBJECTS — The frequency of ingestion of objects like pins, knives, glass, bones, and sharp plastic can vary by culture but is also part of a rare childhood disease, PICU, and done by dare in teenagers and is not very common. Objects that are larger than 25 mm most likely will not pass from the stomach into the bowel and will need to be removed. Objects that become lodged in the esophagus hold the highest risk for perforation and its consequent side effects. These require surgical removal with surgery and/or ENT.
X-rays should be performed to assess the location of the object but remember that not every object can be seen on an X-ray such as wood, some plastic, bone, and glass. Complications of ingestions such as these are perforation of the esophagus with mediastinitis, abscess in the mediastinum, organ penetration, rupture of the aorta, bowel perforation, bowel obstruction or bowel perforation, and death.
Although it seems counterintuitive many times these ingestions can remain asymptomatic for long periods of time making care for them more difficult when recognized.
MAGNETS — Frequency of ingestion of magnets has increased in the last 10 years. These ingestions typically include more than two magnets and although one magnet may be able to pass the GI tract with minimal issue, multiple magnets are more difficult to pass or magnets attached to other foreign bodies. The neodymium magnet found in toys is 5 x more attractive than standard magnets. These are used in toys, body piercings, and facial piercings, and appear on X-ray-like small ball bearings.
Physical examination should concentrate on whether the child has symptoms of bowel obstruction since the batteries can stick together causing a large mass. Emergency endoscopy is the treatment of choice.
In single small magnet ingestion observation and laxative therapy can be utilized. Endoscopy is only indicated when the magnet is large or of unusual shape or pointed that may not pass the GI tract easily. Occasionally, surgical laparotomy may be needed if the magnet is in the terminal ileum to prevent perforation.


ABSORPTIVE OBJECTS — such as toys that grow in water, water beads, diapers, and feminine pads become very dangerous when ingested because they rapidly expand resulting in acute bowel obstruction.
These items are typically not seen on regular X-rays so diagnosis may be delayed. Contrast studies may be performed to confirm the diagnosis but SHOULD NOT delay definitive therapy.
Treatment is an Emergency Endoscopy.