By Santa J. Bartholomew M.D. FAAP, FCCM
Acute Abdominal Pain in Children: Non-Surgical Emergencies
In this second part of our series on Acute Abdominal Pain, we will explore non- surgical causes of abdominal pain that are common in children. Keep in mind that this series of articles is an overview of this topic on which textbooks have been written.
Causes for Non-Surgical Abdominal Pain
Acute abdominal accounts for approximately 9% of visits to physicians’ offices and although we never want to miss a surgical abdomen, they account for 2% of all visits to offices and the emergency department. In a previous article I have outlined the major causes of surgical abdomen including:
- Appendicitis
- Midgut Volvulus
- Intussusception
- Pyloric Stenosis
- Incarcerated hernia
- Hirschsprung’s syndrome
- Meckel’s diverticulum
- Testicular torsion
- Ovarian torsion
Symptoms and signs that increase the risk of illness being surgical in nature are:
- Fever
- Vomiting bile (green vomit)
- Absent bowel sounds
- Tense or rigid abdomen
- Exquisite tenderness when examiner releases hand from abdomen (rebound tenderness)
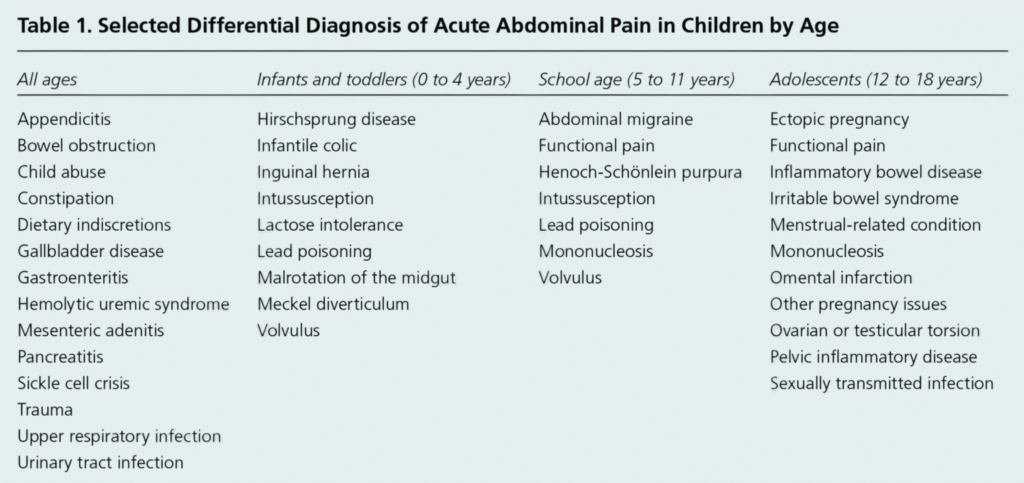
As in Part One, the age of the child can help with differential diagnosis as common causes of abdominal pain vary in different age groups.
Colic
Colicky babies usually cry inconsolably often bringing them to medical attention. There is a predictable diurnal pattern to their crying which usually occurs more in the evening hours. The prevalence of colic is 5-19% and is defined best by Wessel’s criteria of crying for at least 3 hours a day, at 3 days a week for at least three weeks.
The importance of diagnosing and treating colic is excessive inconsolable crying can be frustrating to some caregivers and be a trigger for shaken baby syndrome. It is estimated that approximately 1% of parents of a 1-month-old admit to shaking their child at least once to get the child to stop crying. 2.2% admit to having shaken, slapped or smothered their infant to stop crying. By 6 months of age 6% of parents have admitted to trying these shocking behaviors to get their child to stop crying.
It is estimated that approximately 2.2% of parents admit to having shaken, slapped or smothered their infant to stop crying.

Cow’s milk allergy may play a causative role in portion of formula fed infants there are also infants who experience idiopathic infant colic. There are also theories that infant colic may be akin to abdominal migraine. A highly genetic disorder but theses studies today are all retrospective case-control studies.
Clinical picture:
Inconsolable infant crying usually beginning about two weeks of life. More in the evening than daytime hours suggesting a role of the circadian rhythm in this process.
Treatment:
- Parent education – this is not an illness that anyone causes, it generally ends by three months, how to manage frustration with infant, finding resources for parents when they become overwhelmed.
- Decrease stimulation for the infant
- Turn down loud TVs, music, and remove toys that make noise
- Dim lights and have older siblings and animals who provide stimulation go to another part of the home
- Avoid strong smells such as cooking, perfume, incense
- Rock baby gently, no jiggling
- As sleep seems to be helpful in terminating abdominal migraines anything that encourages sleep in the infant may also be useful.
- Acetaminophen may be helpful when non-pharmacologic treatments fail but must be used as a last resort and prudently when dosing.
Constipation
Constipation is among one of the most common causes for visits to the emergency department. Constipation occurs in 30% of children, peak prevalence between ages 3-5 years old. Although it’s true that functional constipation is responsible for 95% of constipation in healthy children, it is important to evaluate each child for organic causes for constipation.
Constipation defined: fewer than 3 stools a week, fecal incontinence, large palpable stools in rectum or on abdominal examination, pain on stooling.

Other Causes of Acute Abdominal Pain
- Gastrointestinal infections: can cause severe “crampy” abdominal pain and diffuse abdominal tenderness to examination before diarrhea begins.
- Causes: can be viral or bacterial.
- Treatment: is supportive in the cases of viral GI infections but may include antibiotics is stool cultures reveal a bacterial source.
- Urinary Tract Infection: abdominal pain and fever are the classic presenting sign of UTI in children 2 to 5 years old. Infants may also stop feeding and have vomiting.
- Symptoms: foul smelling urine, non-specific signs like fever, irritability, nausea and vomiting
- Treatment: antibiotics
Evaluation and Diagnosis of Acute Abdominal Pain in Children