
By Santa J. Bartholomew M.D. FAAP, FCCM
See Corresponding Case Study: Pediatric Hypoxic Ischemic Encephalopathy (HIE)
Drowning
Drowning is defined as the submersion in liquid causing respiratory impairment. Terms such as near drowning, dry drowning, wet drowning, delayed drowning are all terms no longer used in the literature.
Fatal and non-fatal drownings are responsible for a significant cost to the US healthcare system. Estimated costs of drowning in 2015 were $68.5 million. Drowning is the one of the top 5 causes for death round the world in children 1 to 14 years old, so it is a substantial health risk worldwide.
Risks for Drowning
Age and location of fluid
- 10% of all fatal drowning incidents occur in bathtubs with the highest risk in children under 1 year old.
- 38% occur in pools in the 1- to 4-year-old age group.
- 43% occur in open water and with increasing risk as children grow older. Adolescents are the second only to toddlers in drowning death because of increased risk-taking behaviors in this age group.
Supervision
- A study in Arizona, California and Florida found that 69% of children drowned during NON-SWIM times underscoring the need for appropriate barriers.
- 90% of parents in a survey by Safe Kids Worldwide attested that they consistently supervise children when they are in the water, meaning that most children drown under supervision.
- If supervising adult is distracted talking on phone, texting, social media or impaired by alcohol of drugs children are at greater risk of drowning.
Medical Conditions
- Medical conditions such as epilepsy increase risk of drowning. In fact children with epilepsy have a 10 fold higher risk of drowning than those without epilepsy.
- Children with Autism, Prolonged QT syndrome, other arrythmias are also at increased risk.
Sex and Race
- Boys are twice as likely to drown than girls and it is the leading cause of death in boys worldwide.
- CDC also report a racial disparity in which African- American children ages 5 to 9 years drown in pools at a rate 5.5 times higher than white children of the same age.
Alcohol and environmental factors
- Alcohol plays a significant role in teenage drownings.



Boys are twice as likely to drown than girls and it is the leading cause of death in boys worldwide.
90% of most children drown even under adult supervision.
Alcohol plays a significant role in teenage drownings.
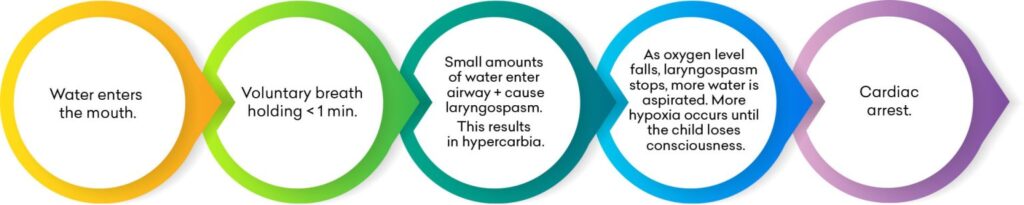
Pathogenesis of Drowning
Children typically drown quickly and quietly, they may slip under the water without a splash or thrashing as depicted by the media. There is an “intrinsic drowning response” in which the autonomic nervous system is triggered making the victim incapable of yelling out or waving their arms. The arms instinctively move to the side to try to lift the body and bring the head out of the water to breathe but because of relatively poor upper body strength this is often not accomplished.
The drowning process generally occurs in 1 minute or less.
Complications of Drowning
Central nervous system
- Hypoxic-ischemic injury to the brain
- Cerebral edema
- Permanent neurologic damage – directly related to the duration of submersion
Pulmonary
- Hypoxemia
- Pneumonia
- Acute respiratory distress syndrome
- Pneumonia
- Non -cardiac pulmonary edema
- Chemical pneumonitis due to aspiration of gastric contents
Renal and metabolic
- Metabolic acidosis: most common metabolic consequence of drowning
- Renal insufficiency
Hypothermia
- Water temperature in which patient was submerged is NOT a factor
Infectious and hematologic
- Sepsis
- Systemic inflammatory response syndrome
- Hemolysis (rare)
- Disseminated intravascular coagulation (rare)
Misnomers for drowning
These are terms used by lay media but not supported by the literature:
- Dry drowning – historically used in cases in which no water was found in lung at autopsy.
- Secondary drowning – describes patients with severe pulmonary edema after insult.
Management
- Initiation of bystander CPR immediately after drowning is the most significant factor in good neurologic outcome.
- Generally recommended to observe patients for 4 to 8 hours monitoring for hypoxia and respiratory distress or altered mentatio
Suggestions for the management of drowning
Pre-hospital interventions
- Bystander cardiopulmonary resuscitation, and
- Initiation of advanced cardiac life support.
In-hospital asymptomatic patients
- Evaluation – pulse oximetry monitoring
- Disposition – discharge after 4 to 8 hours of monitoring
In-hospital symptomatic patients
- Evaluation – may include blood gas, complete metabolic panel, complete blood cell count, chest x-radiography, cardiorespiratory monitoring, pulse oximetry, toxicology testing.
- Resuscitation
- Respiratory support to prevent further hypoxia.
- Volume expansion with intravenous fluids and vasopressors if needed.
- Electrolyte disturbance correction if indicated; however, will likely improve with ventilation, oxygenation, and fluids.
- Remove cold, wet clothing and warm patient to 91.4ºF to 96.8ºF (33ºC to 36ºC.)
- Disposition
- In-patient admission to intermediate care until or ICU for patients with persistent respiratory distress or altered mental status.
Drowning Prevention
- Barriers and fences on all 4 sides of pool.
- Employing a touch supervisor while children are in water. This person is in the water within arm’s length of swimming children
- Water watcher: an adult that is at the pool side without distraction watching swimming children
- Formal swimming lessons beginning 1 year old
- Having all adults (or able-bodied persons) in household learn CPR.
- Some type of flotation device for all children under 6 years old
- Blocking of drain covers so children to not get stuck in drains
- Weight bearing pool covers.



Install barriers or fences around all four sides of the pool.
Floatation devices for all children under the age of six.
Having all able-bodied household members trained in CPR.