By Santa J. Bartholomew M.D. FAAP, FCCM
Kawasaki Disease is an acute, self-limited disease of the blood vessels including the coronary arteries of the heart occurring in infants and young children. It is usually manifested by high fever, inflammation of the mouth, tongue, and eyes (causing peeling and cracked lips, swollen and red tongue and red, swollen but not crusty eyes) and swollen lymph nodes in the neck. The inflammation of this disease also targets the coronary arteries of the heart and other cardiovascular structures. There are diagnostic criteria that assist health care providers in accurately diagnosing Kawasaki disease that have been published by the American Heart Association (AHA) as seen below.
Classic Kawasaki Diagnosis
Classic KD is diagnosed in the presence of fever for at least 5 d (the day of fever onset is taken to be the first day of fever) together with at least 4 of the 5 following principal clinical features. In the presence of ≥4 principal clinical features, particularly when redness and swelling of the hands and feet are present, the diagnosis of KD can be made with 4 d of fever, although experienced clinicians who have treated many patients with KD may establish the diagnosis with 3 d of fever in rare cases.
- Erythema and cracking of lips, strawberry tongue, and/or erythema of oral and pharyngeal mucosa
- Bilateral bulbar conjunctival injection without exudate
- Rash: maculopapular, diffuse erythroderma, or erythema multiforme-like
- Erythema and edema of the hands and feet in acute phase and/or periungual desquamation in subacute phase
- Cervical lymphadenopathy (≥1.5 cm diameter), usually unilateral
Laboratory tests typically reveal normal or elevated white blood cell count with neutrophil predominance and elevated acute phase reactants such as C-reactive protein and erythrocyte sedimentation rate during the acute phase. Low serum sodium and albumin levels, elevated serum liver enzymes, and sterile pyuria can be present. In the second week after fever onset, thrombocytosis is common.
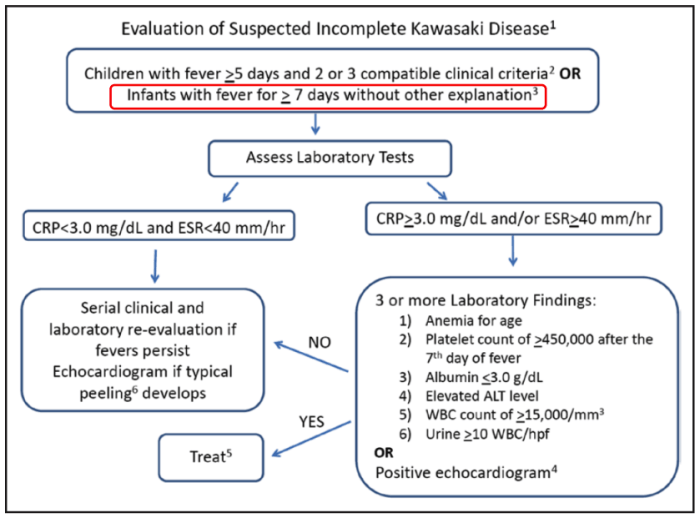
There are also children who may have a “non-classic” presentation and the diagnosis of “Incomplete Kawasaki Disease” has been described in a similar algorithm from the AHA.
Once diagnosis is made echocardiogram is the mainstay of cardiac evaluation in the acute phase looking for coronary artery aneurysms which will affect the morbidity and mortality of the child affected.
There is no one lab test that makes the diagnosis of KD. The mortality and morbidity associated with this disease depends on how quickly the clinical signs are recognized and diagnosis made.
Treatment
The goal of therapy is to abort the inflammatory response and possibly stop thrombosis associated with it. IVIG is the most efficient method to accomplish this and helps diminish the incidence of giant coronary artery aneurysms. IN children with aneurysm at diagnosis antiplatelet therapy is also reasonable.
In children with coronary artery aneurysms the goal of long term therapy is to avoid thrombosis of arteries and ischemic heart disease but the ultimate goal is to recognize this disease early and abort the inflammatory response with IVIG.