By Santa J. Bartholomew M.D. FAAP, FCCM
Rhabdomyolysis
Rhabdomyolysis is a common clinical syndrome that accounts for 7% of acute kidney injury in the USA. As many as 25,000 cases are reported annually in United States. Rhabdomyolysis occurs as the result of an injury to the muscle tissue leading to muscle breakdown and the release of the breakdown by-products into the bloodstream; namely myoglobin but also creatine kinase, phosphate, and potassium, all of which are harmful to the kidney. It can also occur from a wide variety of illnesses or diseases including the four most common:
- Traumatic crush injury, electrocution (i.e., lightning strikes), heat stroke
- Extreme exercise – several factors predispose: concentric contractions such as when running downhill, high humidity, anticholinergic drugs, low potassium and performance enhancing drugs
- Medications – 200 medications account for half of all rhabdomyolysis cases
- Infections
Causes Of Rhabdomyolysis
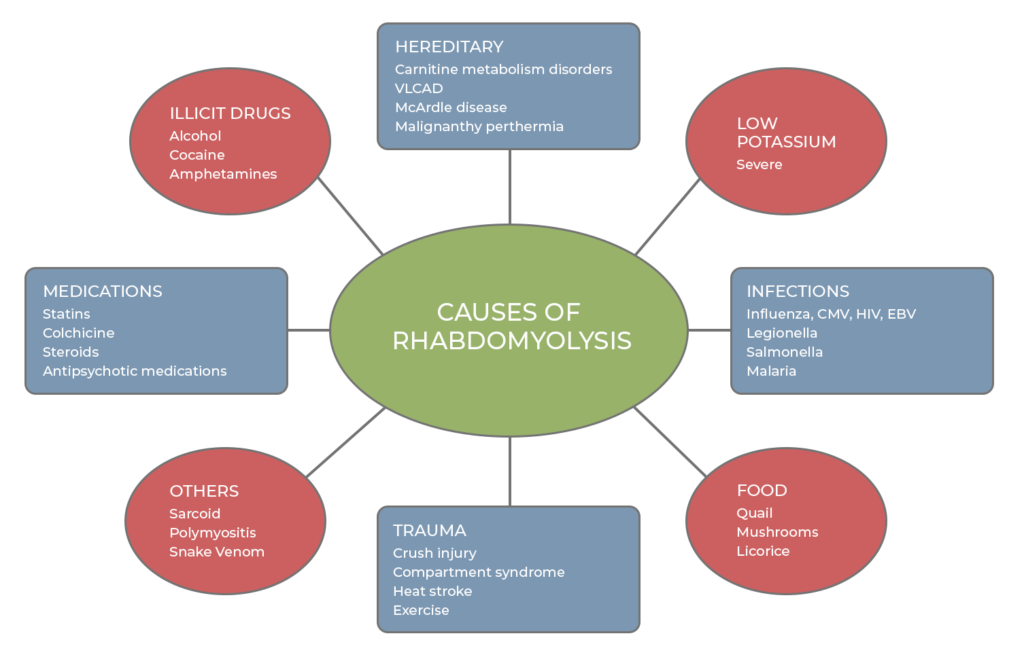
NOTE: If rhabdomyolysis occurs in any patient more than once, then genetic causes need to be investigated.
| DISORDER | GENE |
|---|---|
| β-Sarcoglycan | SGCB |
| Carnitine palmitoyltransferase II | CPT2 |
| Cytochrome (b and c oxidase) | RYR1 |
| Lactate dehydrogenase | LDHA |
| Myoadenylate deaminase | AMPDA1 |
| Myophosphorylase | PYGM |
| Myosin light chain kinase gene mutation | C49T, C37885A |
| Phosphofructokinase | PFKM |
| Phosphoglycerate kinase | PGK1 |
| Phosphoglycerate mutase | PGAMM |
| Phosphorylase b kinase | PHKA1 |
| Very long chain acyl coenzyme A dehydrogenase | ACAD9 |
Clinical Presentation
Most children present with the classic triad however it is important in teens and young adults to assess exposure to alcohol and illicit drugs that can further complicate the renal injury that occurs in ¼ of patients. These children may also have altered mental status.
Older teens and young adults may also present with severe calf pain and muscle swelling that can lead to compartment syndrome if not carefully managed and loss of limb.
Physical examination can give clues to etiology:
- Hepatosplenomegaly on exam may suggest viral infection
- Ptosis and ophthalmoplegia on exam may suggest mitochondrial disorder.
- Nasal congestion, lymphadenopathy, rash may suggest an infectious etiology.
- Proximal muscle weakness may suggest muscular dystrophy
Half of patients present with a clinical triad of:
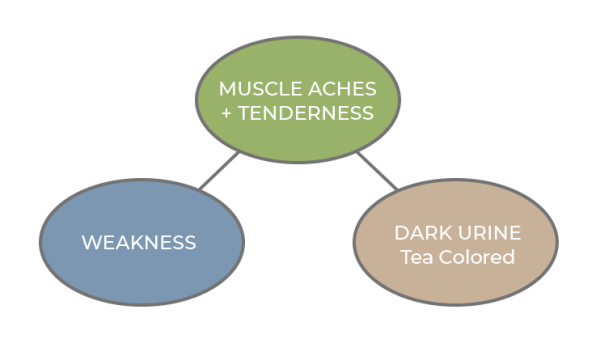
NOTE: If rhabdomyolysis occurs in any patient more than once, then genetic causes need to be investigated.
Pathophysiology of Kidney Injury
- Multifactorial including vasoconstriction, hypovolemia and direct toxicity from the myoglobin and the formation of casts (debris that the kidney usually clears) that clog the kidney filtering system.
- The casts form from the binding of the myoglobin to a protein called Tamm-Horfall protein especially in acidic urine that then clogs the renal tubules
Diagnosis
- Requires a good history and clinical suspicion
- Elevated CK levels: defined by CK >5 times upper limit of normal or > 1,000 U/L
- Supporting lab abnormalities such as elevated LDH, hyperkalemia, hyperphosphatemia and hypocalcemia all point to this diagnosis.
- Final diagnosis is made by quantifying the myoglobin in urine
Treatment
- Aggressive IV hydration: Normal saline is the recommended choice as it contains no alkalinization and no potassium. In children suggested rate is twice maintenance fluids after 20 mls/kg bolus.
- Adult literature suggests goal urine output 3-4 times normal. There are no current pediatric recommendations.
- Stopping all medications that may be implicated in the etiology of the rhabdomyolysis.
- Ruling out drug abuse.
- Early fasciotomy if needed to limit damage to muscle.
- Careful attention to all electrolyte abnormalities.
- CRRT or CRRT-D to remove myoglobin
Although alkalinization and forced diuresis have been used in the past. This was based solely on animal data and retrospective studies and is no longer recommended as part of the care of these children. Neither have been shown superior to aggressive hydration alone.
Complications
- Acute kidney injury: most frequent
- Hypocalcemia early on and the hypercalcemia as kidneys fail
- Hypovolemia from sequestration of fluid in the swollen muscles
- Compartment syndrome: from swelling of muscles
- DIC (late complication)
- Hyperkalemia from release from damaged muscles and decreased kidney function.
Prognosis
- Outcomes vary widely but mortality rates can be as high as 60% in patients that present critically ill.
- Some have suggested increased mortality with initial CK>100,000U/L but there have not been good studies to determine mortality associated with CK levels.